She Did Everything Right. The Data Explains Why It Stopped Working.
What high-performing women over 40 told us, and their answers in the data from the Metabolic Capacity Assessments.
For most of my career, the women sitting across from me were not asking about menopause.
They were asking questions that sounded very different from anything in a standard intake form.
"I don't feel like myself anymore."
"I'm exhausted, but my labs are normal."
"I can still do my job. It just takes so much more effort."
"I used to bounce back overnight."
"I don't know what's wrong with me."
The women saying these things were not failing. They were successful executives, founders, physicians, attorneys, and professionals at the peak of their careers.
From the outside, everything looked intact. Inside, something had shifted. And, every one of them knew it.
They had been to their physicians and their labs were normal.
They had been told it was stress, aging, or a difficult quarter.
Some had tried HRT. Some had added GLP-1 medications.
Some had tightened their nutrition, changed their training, and consulted coaches and specialists.
Most felt somewhat better, but none of them felt like themselves again.
So we built our own measurement:
The Metabolic Capacity Assessment was designed to identify what standard medicine rarely measures: the functional systems patterns creating the gap between being healthy enough to avoid a diagnosis and having the metabolic capacity required to perform consistently at your highest level.
After reviewing the assessment data and interviews from our first wave of respondents, one pattern became impossible to ignore:
The problem was not motivation, discipline, or aging.
No One Scored at the Optimal Metabolic Level
The assessment maps five integrated physiological systems, called the 5 Forces of Metabolic Capacity. They work together and their pattern reveals the root causes behind your symptoms of brain fog, forgetting words, afternoon energy crashes, general fatigue... Each Force is scored from zero to one hundred. A score of 85 percent or above indicates optimal function.
Zero percent of the women assessed reached that threshold. Not the ones who exercise consistently, eat carefully, and prioritize sleep. Not the women who had already tried everything available to them.
The highest score in the group was 84 percent. The average was 64.3 percent, placing the population in Moderate Metabolic Drift: the range where sustained performance is getting harder, compensatory patterns have become habitual, and the gap between what she knows she is capable of and what her system can currently sustain is getting to big to ignore.
If this were simply normal aging, we would expect a random distribution across the spectrum. Instead, we found a consistent pattern. And patterns point to physiology.
0% of high-performing women assessed reached optimal metabolic capacity.
Not because they stopped trying, but because the combined impact of midlife changes with sustained high levels of stress had caused their metabolism to drift.
What the High-Performing Women In Perimenopause and Menopause Told Us
Before we looked at the data, we looked at the language. The way women described what they were experiencing was specific, consistent, and unlike anything in the clinical vocabulary of menopause care.
"I can still perform. I just have to work so much harder at it."
"I need all weekend to recover from the week."
"My brain shuts down at 2 p.m. and I can't think my way out of it."
"I feel like I aged overnight."
"I feel like my body is betraying me."
"I'm doing everything right. Why isn't it working?"
"I stopped going for the big opportunities because I can't count on myself the way I used to."
These are not complaints. They are precise words from women who are skilled at monitoring their own performance. The consistency across women who did not know each other, in different industries, in different roles, describing the same pattern in almost identical language, was the first signal that we were looking at something systematic.
What the Metabolic Capacity Assessment Data Revealed
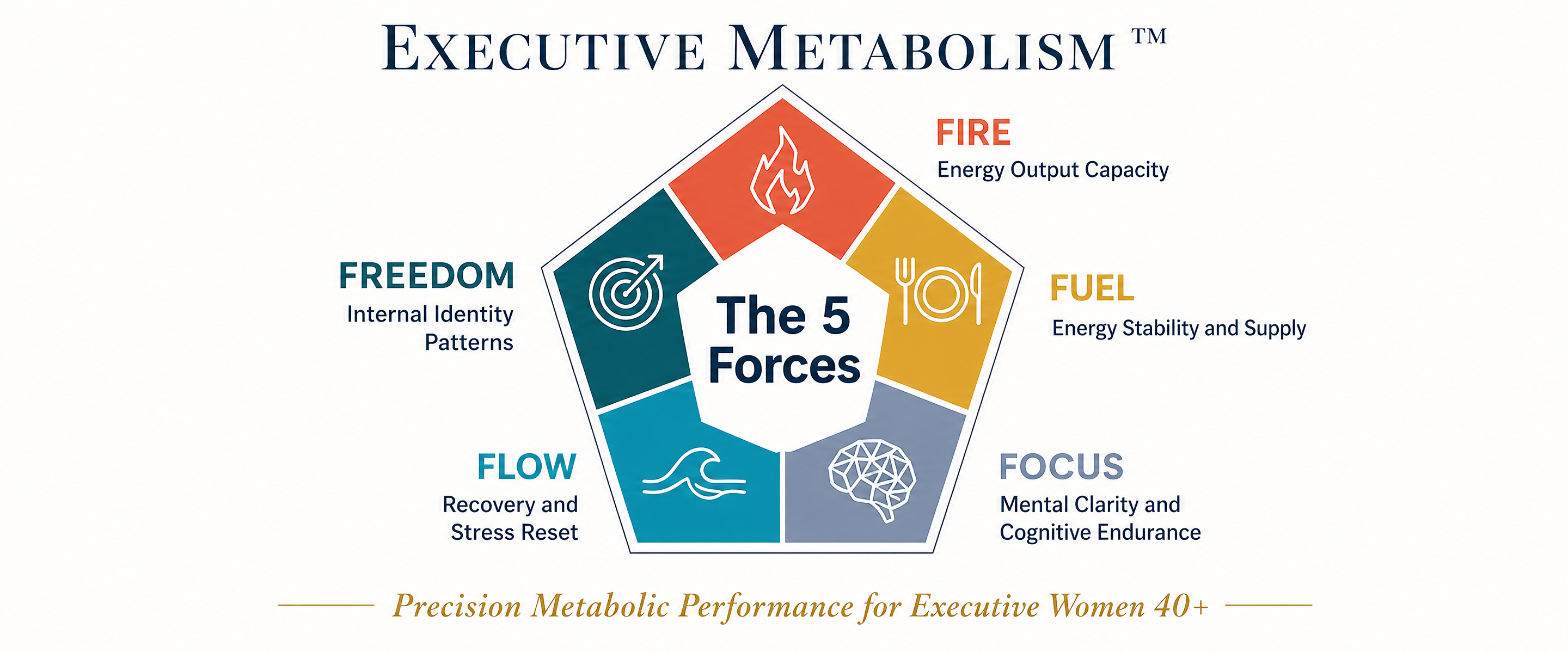
The assessment measured five biological systems that govern performance capacity. Here is what the data showed across each Force, and what it looks like from the inside.
FIRE — when the body stops keeping the agreement
She is training the same way she has for fifteen years: same discipline, same program, same effort. Belly fat is increasing anyway. The recovery after a hard week stretches from one night to two days. She has adjusted her expectations so gradually that she has stopped noticing how much ground she has given up.
Eighty four percent of women in our cohort said their body composition has stopped responding, despite their efforts. Estrogen supports the proteins that regulate mitochondrial efficiency. When this declines, your cellular power system produces less energy. The same input produces less output.
84% say their body composition has stopped responding to the same effort.
Same discipline, same training, same nutrition. Different results. This is not a calories in-calories out problem.
FUEL — good nutrition that is not hitting it's target
She eats well. She has been intentional about food for years. She still craves sugar most evenings and cannot fully explain it. She starts the day with coffee before food and tells herself she will eat when she is hungry.
Fifty two percent of our cohort do not start the day with a protein-forward meal.
Thirty two percent experience frequent digestive symptoms they have largely normalized and stopped mentioning to anyone.
Evening cravings are not a willpower failure. They are a glucose stability signal. The body is reaching for quick fuel because the fuel and nutrient delivery system has become less consistent across the day. (Read more about how glucose stability and insulin performance optimization impact performance.)
52% don't start the day with a protein-forward meal.
Perimenopause changes our relationship to cortisol, the stress hormone. A high-protein morning snack or breakfast shortly after waking helps manage cortisol and improve our blood sugar stability throughout the day.
FOCUS — the word that disappears
She was mid-sentence in a presentation she had given twenty times. The word was just gone. She found a different word, kept moving, finished without anyone noticing.
But she noticed. And then she started keeping her own record after that: the words that went missing in rooms, the names she reached for and missed, the sentences that lost their thread before she finished them. She had not told her doctor. She was afraid of what it might mean.
Fifty eight percent of the women in our cohort said they arrived at work the morning after a demanding day still not feeling fully recovered.
The brain consumes roughly 20% of the body's glucose, with the prefrontal cortex, which governs word retrieval, decision-making, and strategic thinking, among its most metabolically expensive structures. (Read more about how glucose usage impacts cognition.)
When insulin precision drifts in perimenopause, glucose delivery to that region becomes inconsistent. Word recall fails, and brain fog episodes increase. This unreliability is its own kind of frightening for a woman who has built her career on precision.
58% arrive at work after a demanding day not fully cognitively recovered.
Their best decision-making window is narrowing. Most of them have no clinical framework for why.
FLOW — the off switch that stopped working
She does everything right at night. Consistent bedtime, no screens, good habits she has maintained for years.
She wakes at two in the morning anyway, her mind already running tomorrow's agenda. She lies there for an hour, composing meetings she has not yet attended, before she gives in and reaches for her phone.
She is not anxious. She does not have insomnia. Her nervous system has lost some of its capacity to fully stand down. She is stuck in Protection Mode.
Seventy three percent of our cohort do not wake feeling rested, even after a full night of sleep.
Forty four percent experience the wired-but-tired state often.
Estrogen directly supports the parasympathetic nervous system, the system governing genuine recovery. When it declines, the signal that tells the body it is safe to let go becomes weaker. Sleep hygiene can help, but The FLOW Force addresses the root cause of it.
73% do not wake feeling rested, even after a full night of sleep.
The nervous system isn't winding down to make it safe to rest deeply. It stays in a semi-alert state all night, draining the energy sleep is meant to restore.
FREEDOM — the beliefs and narratives that govern our capacity
FREEDOM is the strongest Force in the group, averaging 76 percent. And it is the most important number in the entire dataset.
Fifty eight percent of the women assessed instinctively deflect or minimize genuine compliments.
Fifty seven percent still feel guilt when they slow down. It is the single most prevalent behavior across the whole assessment.
Here is what the data is saying: the drive and ambition are intact. The standards these women hold have not softened. What has drifted is the physiological infrastructure running underneath all of it. The body has moved into a Protection Mode that is working against her, because the woman who is in it does not know it's been activated.
She is not losing her edge. Her metabolism changed and nobody gave her a map.
57% feel guilt when they slow down.
The most prevalent behavior in our entire dataset. This single pattern impacts whether or not we will commit to the self-care habits that can sustain our performance levels.
Why Women Experience Inconsistent Results
The women in this data had tried to fix their problems. Many had tried HRT, GLP-1 medications, supplements and adaptogens, intermittent fasting, biohacking strategies, and high-performance coaching.
The question is not whether any of those work. Many of them do, but when we play a guessing game based on something we read, or that a friend recommended, we aren't applying the protocols our specific pattern needs.
The question is whether the intervention addresses the primary imbalances in a specific woman's specific pattern.
HRT addresses hormonal deficiency and has genuine relevance to the FIRE and FOCUS Forces for many women. It does not recalibrate accumulated autonomic dysregulation. A woman on HRT whose FLOW Force is still in significant deficit may find her sleep partially improved and her brain fog unchanged. The intervention wasn't made for the pattern.
GLP-1 medications address appetite signaling and can provide meaningful FUEL and FIRE Force relief for some women. For women whose primary deficit is in FOCUS or FLOW, a GLP-1 changes one variable in a five-variable system.
General wellness interventions, better sleep, cleaner nutrition, more consistent training, are not wrong. They are undifferentiated and often based on data from men or younger women, not for her age and stage of life.
Applied without knowing which Forces are in deficit and in what sequence they are affecting each other, they produce the partial results most of these women have already experienced.
Assessment before protocol. Precision before effort. The intervention order determines the ROI.
The Invisible Tax
The most expensive consequence of unaddressed Metabolic Drift is not the fatigue or the brain fog, as real as those are.
It is the decisions we make when we don't feel confident in our capacity to show up with 100% and succeed.
- The hand that does not go up in the room.
- The idea not pursued.
- The proposal not submitted.
- The conference not attended because the recovery math did not work out.
- The conversation not started because she was not sure the version of herself who could handle it would show up that day.
- The weekend family plans not made because more recovery time was needed.
The women in our assessment cohort were not failing. They were compensating.
The compensation had become so habitual, so quietly woven into how they arranged their professional lives, that most of them had stopped registering how much smaller the life had become.
"I stopped going for the big opportunities because I couldn't count on myself the way I used to."
That sentence is not due to a poor work ethic. It is due to Metabolic Drift.
The assessment data shows it clearly: the ambition is intact, the drive is intact, the standards are intact. What shifted is the physiological reliability underneath them. When a high-performing woman cannot trust her own output, she stops betting on herself in ways that are quiet enough that nobody notices, including her.
The career cost of this pattern accumulates over years. It shows up as the gap between the role she is in and the role she was capable of.
The Most Common Mistake
When Metabolic Drift is significant enough to impact performance, most high-performing women do what they have always done when a problem requires solving: They try harder.
More training. Stricter nutrition. More rigorous sleep habits. Earlier mornings. Additional supplements. A different coach.
But, it doesn't work.
For a woman in Moderate to Sever Metabolic Drift, adding demand to a system in Protection Mode is like throwing gasoline on a fire; the body reads additional training load as additional threat. Caloric restriction signals scarcity to a system already conserving.
The drive that built her career becomes the mechanism that prevents her recovery.
The problem is not the effort. The effort is admirable and consistent. The problem is applying the right general approach to the wrong specific starting point.
Two women with identical symptoms can have completely different patterns. The woman whose FLOW Force is driving her FOCUS symptoms needs a completely different first intervention than the woman whose FOCUS deficit is primary. For example, she needs a nervous system protocol rather than an insulin optimization protocol. Applied to the wrong Force first, even effective interventions produce partial, temporary results.
This is why assessment before protocol is the approach that produces lasting change.
What Normal Labs Cannot Show
Most of the women who took the Metabolic Capacity Assessment aren't "sick", but their metabolic capacity is decreased. None of this would register on a standard blood panel.
Standard medicine measures disease thresholds. A fasting glucose of 94 is normal. Working memory that affects daily performance is "normal" for her age. Body composition changes (stubborn belly fat) that no longer responds to consistent effort is "normal".
She leaves the appointment reassured, but still knows that something has changed.
Normal and optimal are not the same standard. We deserve optimal.
You Are Not Broken
The research published by the Harvard Business Review in 2025 found that women leaders who received appropriate support during perimenopause did not simply maintain their performance, hey emerged more resilient, more strategic, and more effective than before.
This didn't happen despite the transition, but because of it.
The women in this assessment data are in the window where that outcome is still available to every one of them. The lower the level of Metabolic Drift, the easier and faster performance is restored and protected.
The assessment is not a diagnosis, it's a map. It shows your current level of Metabolic Drift and where each woman's system is compensating across all five Forces, which Force is applying the most constraint, and what the starting point for recalibration looks like, specifically for her. There are 125 potential patterns identified in the assessment.
Where to Start
If you recognized yourself anywhere in this article, the Metabolic Capacity Assessment is the first step to take.
It maps all five of your Forces and identifies your Metabolic Drift Level. Not where your symptoms are loudest. Where your system has actually shifted, and in what sequence to address it.
Five minutes. Free. Results are immediate.
Start the Metabolic Capacity Assessment
Frequently Asked Questions
What is the Metabolic Capacity Assessment?
A clinical screening instrument that maps five interconnected physiological systems: FIRE, FUEL, FOCUS, FLOW, and FREEDOM. It generates a score for each Force and an overall Metabolic Drift Level — how far a woman's system has moved from optimal performance capacity and in which direction the cascade is running.
Is this the same as burnout?
Burnout describes a psychological and behavioral state that resolves when the circumstances causing it change. Metabolic Drift is a physiological pattern that persists even when circumstances improve. A woman who takes a real vacation and comes back only marginally rested is not experiencing burnout. She is experiencing a system in Protection Mode. The two can coexist, but they require different interventions.
How is this different from what HRT addresses?
HRT addresses specific hormonal deficiencies and has genuine relevance to several Force deficits, particularly FIRE and FOCUS. It does not recalibrate accumulated autonomic dysregulation, accumulated stress-imprint patterns, or nutritional delivery failures. A woman on HRT who still reports brain fog, slow recovery, or unreliable energy is likely experiencing Force deficits that hormonal support alone does not address. The two approaches are complementary, not competing.
Can I have Metabolic Drift if I am not yet in menopause?
Yes. Perimenopause, which typically begins in the early-to-mid 40s, often years before irregular periods, is the period of greatest metabolic disruption. Many women experience their most significant drift during perimenopause, before a clinical menopause diagnosis.
Why did zero women score optimal?
Optimal metabolic capacity requires 85 percent or above across all five Forces. The average in our cohort was 64.3 percent. This does not mean these women are sick. It means their performance systems are operating below optimal capacity in ways that standard labs are not designed to detect.
About the Author
Stacy Naugle, M.Ac., EAMP. is the Founder and Chief Metabolic Strategist of Executive Metabolism™, a precision metabolic advisory firm for high-performing women over 40. She has 35 years of clinical experience and developed the 5 Forces of Metabolic Capacity framework.
*This content is educational and informational. It does not constitute medical advice, diagnosis, or treatment.
References
-
Klinge CM. Estrogenic control of mitochondrial function and biogenesis. Journal of Cellular Biochemistry. 2008;105(6):1342–1351. doi:10.1002/jcb.2193.
-
Ramesh SB, et al. Heart rate variability as a function of menopausal status, menstrual cycle phase, and estradiol level. Physiological Reports. 2022;10(10):e15298. doi:10.14814/phy2.15298
-
Hellestad Nygård M, et al. Peripheral insulin resistance attenuates cerebral glucose metabolism and impairs working memory in healthy adults. npj Metabolic Health and Disease. 2024;2:19. doi:10.1038/s44324-024-00019-0
-
Rasgon NL, et al. Insulin resistance and medial prefrontal gyrus metabolism in women receiving hormone therapy. Neurobiology of Aging. 2014;35(12):2588–2594. doi:10.1016/j.neurobiolaging.2014.05.010
-
Frontiers in Cardiovascular Medicine. Estrogen deficiency is associated with decreased cardiac vagal control and increased sympathetic tone. 2024. doi:10.3389/fcvm.2024.1402086
-
Grandey AA, Decker M, Barnes-Farrell JL, Stockdale MS. New research on how women in leadership navigated menopause. Harvard Business Review. November 3, 2025.
